When a School’s Multi-Tiered System of Supports Needs Support:
How Do You Motivate Educators and Avoid Educational Malpractice?
[To listen to a synopsis and analysis of this Blog on the “Improving Education Today: The Deep Dive” podcast on Spotify. . . hosted by popular AI Educators, Angela Jones and Davey Johnson: CLICK HERE for Angela and Davey’s Enlightening Discussion]
Dear Colleagues,
Introduction
It’s been an MTSS kind of week.
MTSS. . . as in a Multi-Tiered System of Supports.
As in the continuum of academic or social, emotional, behavioral services, supports, or interventions to help students succeed in their general education classrooms.
As in the system that is required of every school by the Elementary and Secondary Education Act (ESEA, 2015) as follows:
“a comprehensive continuum of evidence-based, systemic practices to support a rapid response to students’ needs, with regular observation to facilitate data-based instructional decision-making.”
As in “multi-tiered system of supports”. . . because the term is only written in lower case terms in ESEA’s federal law, without any capital letter “MTSS” acronym.
Meaning. . . that Federal Law does not require any district or school to use the (upper case) MTSS approaches “suggested” (even though it doesn’t feel that way) by the U.S. Department of Education, any of its tax-funded National Technical Assistance Centers, or most State Departments of Education.
_ _ _ _ _
But that’s not why it was an MTSS week.
It was an MTSS week (like many other weeks) because yet another company. . . unabashedly marketing its services. . . issued yet another White paper. . . to “help” schools design and implement (their—that is, the Company’s) “effective” MTSS services.
This week, the White paper discussed how to overcome the “barriers” to MTSS. . . without, as usual, describing (a) any field-tested and proven MTSS processes, (b) implemented in multiple schools under multiple conditions, (c) that were objectively shown to work across multiple sites and years.
Which begs the question:
“Wouldn’t you rather know how to implement effective and proven multi-tiered systems of support before discussing how to address the barriers. . . that may be occurring because you never started off with a sound system to begin with?”
_ _ _ _ _
It also was an MTSS week because I had a running LinkedIn conversation with a polite and seemingly honest “connection” who wanted to interview me on effective MTSS processes.
Long story short: he was a salesperson (literally the description on his LinkedIn profile) with a degree in Business who had a contract with a major university that wanted his help to develop “MTSS technology” that schools could use to find the “right” academic interventions for its struggling students.
Whew. . .
After validating that he wasn’t going to “bait and switch” me on the phone call to sell me something, he eventually admitted (through our LinkedIn interchange) that he knew nothing about MTSS and needed to learn “from an expert.”
I respectfully and politely begged off. . . explaining that I did not want to (potentially) compete with myself. . . if they actually developed this technological application and had beaucoup bucks (which I don’t) to market it.
The point is: There are too many “educational” companies that market well, but deliver poorly. . . on behalf of our students, staff, and schools. . . because (a) they don’t have the expertise to “know what they do not know,” and (b) their “good intentions” are not grounded in science, objective evaluation data, and proven practices.
Indeed, there is a reason I do not practice medicine. . .
It’s because I am not trained as a medical doctor.
I’m not going to interview a bunch of doctors, and then head into surgery to begin to practice (literally).
A Scary Medical Diversion
Speaking of medicine, let’s turn to a couple of medical metaphors that are, indeed, scary.
- Scenario 1. You have a medically fragile child with a serious chronic condition. Having just moved to a new community, you are interviewing a new specialist. You are sitting down with one who exclaims, “I never look at my new patients’ medical histories. We will need to re-establish your child’s medical baseline with new tests, diagnoses, and perspectives.”
You have spent years and thousands of dollars to identify your child’s condition, to medically stabilize it, and to help her to thrive.
What do you say to the doctor you are interviewing?
_ _ _ _ _
- Scenario 2. You bring your child to the Emergency Room with a serious, but not life-threatening, puncture wound. After talking with the in-take attendant, you sit in the Waiting Room which is filled to capacity until being called into a treatment cubicle.
After a long period of time, an attending nurse and doctor appear, telling you, “It’s been a busy night, and we are understaffed,” then asking you briefly “What happened?” The doctor proceeds to immediately inject your child with an unknown medication, and they both leave. No one has asked about your child’s medical history or allergies.
Your child immediately breaks out in hives, and begins to have breathing problems. What do you do. . . short-term and long-term?
_ _ _ _ _
- Scenario 3. Your elderly parent has been hospitalized for weeks for a chronic, untreatable condition that will eventually result in death. Based on her Living Will, she is receiving minimal levels of medication, treatment, and life-sustaining support.
One evening, you leave the hospital to get some food and take a break. When you return, your mother is surrounded with monitors and doctors, medication is being pumped into her I.V., and she is about to have her heart shocked.
You later find out that no one on the new shift read her chart with the “Do Not Resuscitate” orders.
How do you react?
_ _ _ _ _
I would have to imagine that you are reacting to the three scenarios above with a mixture of shock, rage, and disbelief.
And I share those emotions.
All three situations involve inexcusable breaches of medical protocol and care, and each require response, remediation, and accountability. . . if not considerations of medical malpractice.
Hold that thought. . .
The MTSS “First Things First” Protocol
Mid-way through my career, I was the Director of the Arkansas Department of Education’s federally-funded State Personnel Development Grant.
In this capacity, I oversaw both the MTSS and PBIS implementation systems for the State for 13 years, and we developed approaches that were grounded in (school) psychologically-based research-to-practice.
These practices significantly improved on the special education-framed (and often flawed) MTSS and PBIS approaches coming out of the U.S. Department of Education’s Office of Special Education Programs (often through State Departments of Education like mine).
Relative to MTSS, we developed an implementation Flow Chart that guided schools when they had students demonstrating significant or persistent academic struggles and/or social, emotional, or behavioral challenges. At different points in the Flow Chart, there were decision junctures where teachers, related services professionals, or multidisciplinary MTSS Teams needed to apply collected data in order to decide where to go next.
The entire Flow Chart and MTSS process was field-tested before we implemented it across the State. And, our data demonstrated that students received more effective services, supports, and interventions in more time- and cost-effective ways, and that targeted student outcomes were more often attained.
_ _ _ _ _
Toward the beginning of the protocol. . . in Step 2, when general education teachers identify, early on, significant concerns about a student. . . we recommended a series of data-collection activities that we call the First Things First.
The goal of these activities is to get a complete current and historical picture of the student so that we can identify the “Relevant Known,” “Relevant Unknown,” and “Irrelevant” pieces of information related to the student’s existing (and past) concerns.
- The Relevant-Known information is actively considered as we complete root cause analyses to determine the underlying reasons for a student’s concerns.
- The Relevant-Unknown information involves missing information that must be found, determined, or collected, and integrated into the root cause analysis before any interventions are considered.
- And, the Irrelevant information is set aside so that it cannot bias, mislead, or “contaminate” the root cause analysis process or its outcomes.
In many ways, the First Things First activities are no different than a doctor or nurse getting a patient’s medical history and current medical status.
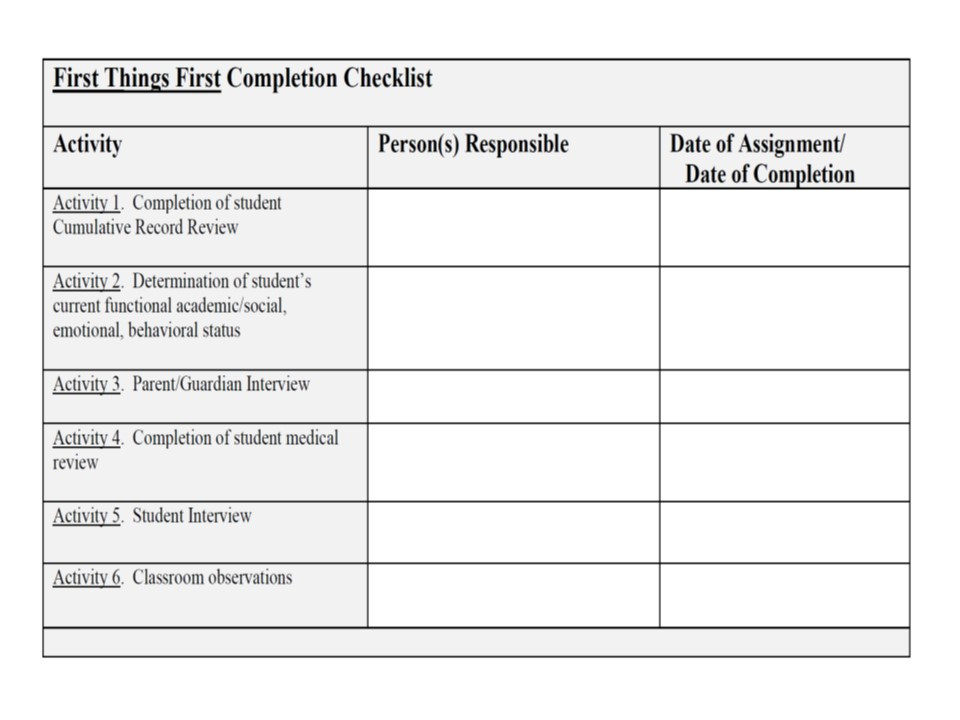
Briefly, the First Things First activities include (see also Table 1 below):
- Activity 1. Complete a Cumulative Record Review on the student. This involves synthesizing information on the schools attended by the student and his/her yearly attendance; student grades and test scores; services, supports, and previous interventions; medical, health, and family history; social, emotional, behavioral, and school discipline history; and other important factors related to the student’s school functioning.
_ _ _ _ _
- Activity 2. Determine (with other teachers, consultants, or school personnel, as needed) the current, functional academic and behavioral status of the student. This involves identifying the academic and behavioral skills that the student has mastered (regardless of the “grade level placement or designation” of those skills), the current instructional level of the student, and the student’s “frustration” level—that level where material is currently too difficult for the student to learn.
_ _ _ _ _
- Activity 3. Interview the parents/guardians, last year’s teachers or teaching team, previous years’ teachers or support personnel, and anyone else of relevance to discuss the student’s strengths, weaknesses, development, and progress—especially as it relates to the areas of concern. All of these interviews are documented on a Case Contact Log.
_ _ _ _ _
- Activity 4. Determine the need for social, developmental, or medical assessments of the student—decisions that may involve other school personnel (e.g., the school nurse, counselor, school social worker or psychologist).
Such assessments may include: (a) a formal Social-Developmental History or Assessment, and/or (b) Health Screenings, Medical Check-ups, or other Physical/Physiological Diagnostic Assessments. In this latter area, it is important to identify (or discount) the impact of any student-specific medical, physiological, neurological, biochemical, or other issues that exist and may be affecting students’ academic or behavioral status or progress.
_ _ _ _ _
- Activity 5. Interview the student (as age-appropriate) to determine his/her perspective of his/her academic, behavioral, and other strengths, weaknesses, challenges, and/or concerns.
_ _ _ _ _
- Activity 6. Have a skilled colleague come into the classroom (or the setting where the concerns are occurring) to complete systematic observations of the student relative to their academic and/or behavioral engagement, student-teacher-instructional-curricular interactions, and reactions/responses to different circumstances or conditions.
_ _ _ _ _
Should the MTSS First Things First Protocol Be Voluntary? A Case Study
As a consultant working with districts and schools across the country, I am constantly sharing the MTSS Flow Chart (or colleagues purchase it in our MTSS Guidebook, or MTSS Design and Implementation On-Line Course).
As part of the training, we eventually complete Case Studies together using real students who are demonstrating academic struggles or behavioral challenges. . . both to practice (with me serving as a coach and mentor) the MTSS process, and to complete the needed root cause analyses that are then linked to service, support, and intervention recommendations.
_ _ _ _ _
A recent Case Study involved a young lady in Grade 8 who was taking advanced early-High-School courses, but was struggling in some of these courses, was missing assignments, and was experiencing high levels of anxiety. She was on a medically-related 504 Plan for some gastro-intestinal issues, she was not sleeping, and there was a history of Attention Deficit Disorder.
Academically, she was reading at an early High School level, but her assessments suggested that she did not always understand the more complex, higher-ordered nuances of some passages. Mathematically, she was “Below Basic” especially in algebraic functions, measurement, geometry, and fractions, but her math grades were A’s and B’s.
While it would be natural to wonder if the medical, sleep, anxiety, and missing work issues were related to her taking advanced courses, the MTSS Team still needed to complete the First Things First activities and protocol. . . avoiding the inclination of playing what we call “Intervention Roulette.”
Indeed, the Team needed to avoid the mistakes that the medical people made in the three scenarios described above:
- Not considering the student’s psychoeducational history, past assessments, and confirmed conclusions (Scenario 1);
- Not interviewing the parents to get the most complete perspectives of the student’s past and current status (Scenario 2); and
- Not reading the complete 504 Plan and all of the medical and psychoeducational assessments related to it, as well as all relevant meeting notes and deliberations.
Critically, when this student’s entire Cumulative Record was catalogued, there was no data or information on her Third or Fourth grade years. Moreover, the MTSS Team needed to investigate what she was taught and learned virtually during her Fifth grade “pandemic year.” And, they needed to determine why she moved from one school to another more demanding school at the beginning of Grade 6.
In addition, there was nothing in the records, regarding when her Attention Deficit Disorder was first diagnosed, why she was receiving “Executive Management Skill instruction” from an Occupational Therapist during her current Eighth-grade year, and how her after-school tutoring was linked to her core instruction.
Finally, there was a note in the Records about her anxiety, suggesting that it had been present for a long period of time, and that it was “of significant clinical concern.” And yet, it appeared that the need to get an independent psychological assessment and—potentially—outside therapy had not been fully discussed with the parents. . . as part of the MTSS process.
_ _ _ _ _
Clearly, a number of First Things First activities still needed to be completed before the MTSS Team would be ready to convene and discuss the case.
But. . .
- What if this student’s general education teachers refused to participate in these First Things First activities because “it was not their responsibility”?
- What if the MTSS Team convened, staffed the Case, and proceeded with interventions. . . only to receive First Things First information later on indicating that the earlier interventions were contraindicated.
- And what if these interventions not only did not work, but made the student even more anxious, more resistant, and academically further behind than when they started?
_ _ _ _ _
In the end, these case-specific questions generate more systemic questions:
- Should staff “be allowed” to abdicate from their responsibility (to students, their current and “next-school-year” colleagues, and themselves) to fully participate in MTSS First Things First activities?
- Should staff be held professionally accountable either for not participating in the MTSS process or for not following MTSS protocols with fidelity?
- Should staff be cited, like doctors and nurses, for “Educational Malpractice” when they have consciously and egregiously violated MTSS protocols and psychoeducationally harmed students?
_ _ _ _ _
As alluded to above, multidisciplinary MTSS Team Meetings should not be held until the First Things First activities are completed. This reasonably assures the Team that all of the existing information and data on the student-of-concern will be “at the table” and available for discussion and analysis.
Using a different metaphor, the First Things First activities are similar to the “Discovery” process whereby lawyers dig through, sift, and analyze all of the available information that is relevant to a case. Indeed, lawyers rarely begin a trial without methodically completing the Discover and Deposition process. Lawyers do not like it when case information is missing, or it unpredictably emerges when a witness is on the stand.
While completing the First Things First activities ensures that the existing data and information are available at the (first) MTSS Team meeting, the data-collection process also gives different MTSS Team members an opportunity to work collaboratively with students’ general education teachers to validate that (a) classroom interventions are not working, and (b) an more comprehensive MTSS Team meeting is needed.
Critically, an MTSS Team Meeting involves a lot of people, a lot of collective time, and a lot of coordination. It makes no sense to convene an entire multidisciplinary MTSS Team when there are so many significant First Things First information gaps that no in-depth discussions can occur and no legitimate, data-driven decisions can be made.
When essential Relevant-Unknown information is acknowledged at an MTSS Team Meeting, there are only two appropriate things to do:
- Suspend the meeting and reconvene it when the Relevant-Unknown information is Relevant and Known; and
- Agree that no future MTSS Team Case Meetings will be held unless the Chair has validated that all First Things First activities have been completed.
Said a different way: When critical information is missing at an MTSS Team Meeting, the Team should not engage in Intervention Roulette. . . because that (a) results in low probability of success interventions, (b) low levels of problem resolution and student success, and (c) high levels of potential of Educational Malpractice.
Moreover, if the information gaps are because specific staff are abdicating their MTSS responsibilities, they need to be held administratively accountable.
End. Of. Discussion.
Summary
The MTSS process begins in the General Education classroom with effective differentiated instruction, taught by professionally-prepared and supervised teachers, with research-proven curricula, supported by sound classroom organization and behavior management, and—as needed—data-driven remediation, accommodation, modification, or classroom-based intervention approaches.
The MTSS process is an educational process. It is not a special education process.
When the criteria immediately above are met, schools tend to have few instructional and/or curricular student “casualties.”
_ _ _ _ _
When we consult with districts and schools to upgrade or implement effective MTSS processes, we often begin by discussing, modifying, and agreeing on fourteen core science-to-practice Principles.
Along with the Flow Chart discussed above, these establish the consensus, commitment, and pathways needed for student, staff, and school success.
These Principles are:
Principle 1. Students succeed academically and behaviorally because of the characteristics, actions, interactions, and activities within the Instructional Environment (i.e., the general education classroom).
_ _ _ _ _
Principle 2. Students receive scientifically- and/or research-based instruction to the greatest extent possible in general education settings using grade-level (if possible) general education curricula.
_ _ _ _ _
Principle 3. Instruction focuses on both academic achievement and mastery, and social, emotional, and behavioral self-management and competence. Instruction is differentiated to maximize students’ speed and degree of mastery.
_ _ _ _ _
Principle 4. Student success is most facilitated within positive, safe, and supportive school settings and classroom environments.
_ _ _ _ _
Principle 5. Students’ academic and behavioral progress is continually monitored in the classroom using authentic and other information- and skill-based assessments to determine skill mastery, independence, and application.
_ _ _ _ _
Principle 6. Assessments of student progress are reliable and valid, and they evaluate the functional and meaningful outcomes and proficiencies that relate to curricular, district, and state academic expectations.
_ _ _ _ _
Principle 7. Teachers and others use classroom performance and progress monitoring data as the basis for all instructional decisions.
_ _ _ _ _
Principle 8. When individual students are not making appropriate academic or behavioral progress, the presence of effective classroom instruction and classroom management is evaluated first before considering more specialized or intensive instruction or intervention.
_ _ _ _ _
Principle 9. Teachers and others use a data-based functional assessment process when students are not responding to effective instruction or classroom management to determine whether (a) adapted classroom instruction (e.g., skill remediation, instructional accommodations and/or curricular modification), or (b) more targeted or specific classroom-based intervention is needed.
_ _ _ _ _
Principle 10. When students do not respond to classroom-based instructional or intervention approaches, teachers and others use more intensive, multi-factored, multi-disciplinary data-based functional assessments to determine the root causes and the need for more strategic or intensive services, supports, strategies, and/or programs.
These assessments determine why the student challenge is occurring, and the outcomes are directly linked to the instruction or intervention needed.
_ _ _ _ _
Principle 11. Collegial consultation is provided in the setting(s) where the situation or problem is occurring whenever possible to assist classroom teachers in problem-solving, functional assessment, and/or classroom intervention planning.
_ _ _ _ _
Principle 12. All instructional or intervention services are delivered, to the greatest degree possible, in general education settings or in the settings where the situations or problems are occurring in.
_ _ _ _ _
Principle 13. Instruction/Intervention plans should be written prior to implementation, and they should include the methods and steps, resources and training, timelines and outcomes, and formative and summative evaluations needed for implementation integrity and success.
_ _ _ _ _
Principle 14. Evaluations should be formative and summative and address both short- and long-term intervention goals and outcomes.
As in Alice in Wonderland,
“If you don’t know where you’re going, any road will get you there.”
The only problem is. . . if you take “any” road, you probably won’t get where you really want to go.
Similarly. . . as I used to remind my staff at the Arkansas Department of Education,
“You don’t get credit for being here. You get credit for producing here. . . producing meaningful student, staff, and school outcomes.”
_ _ _ _ _
In summary, this Blog focused on the multi-tiered systems of support process, first emphasizing that:
- It is required for all districts and schools by the Elementary and Secondary Education Act (ESEA, 2015);
- It should be locally designed to link the specific academic and/or behavioral needs of district students to a continuum of multi-tiered resources, professionals, and services, supports, and interventions;
- The U.S. Department of Education’s and your State Department of Education’s MTSS framework is not mandated; and
- Field-proven, science-to-practice procedural flow charts and protocols should anchor the MTSS process, facilitating its implementation consistency and fidelity.
The Blog next described three “medical malpractice” scenarios involving situations where (a) a doctor refused to consider a medically-fragile child’s previous diagnoses and history; (b) emergency room personnel did not interview a parent regarding a child’s existing allergies; and (c) a hospital floor’s staff attempted to resuscitate an elderly patient with a “Do Not Resuscitate” order on a chart that was never read.
We noted that anyone experiencing the negative outcomes of these situations would likely believe that medical malpractice had occurred.
We then detailed a series of specific MTSS activities (called the “First Things First”) that should be completed before any Student Case is presented to a school’s MTSS multidisciplinary building-level Team. These activities are:
- Activity 1. Completion of a student Cumulative Record Review
- Activity 2. Determination of the student’s current functional academic and social, emotional, behavioral status
- Activity 3. Completion of Parent/Guardian and School Personnel Interviews
- Activity 4. Completion of student Medical and Social-Developmental Review
- Activity 5. Completion of a Student Interview
- Activity 6. Classroom observations
A brief Case Study was presented with a number of First Things First activity and information gaps. We discussed how these gaps would affect an MTSS Team’s functioning and deliberations, and wondered what should be done if the gaps occurred due to staff negligence.
Tying the entire Blog together, a final question posited, “Should school staff be cited, like doctors and nurses, for “Educational Malpractice” when they have consciously and egregiously violated MTSS protocols and harmed students?”
_ _ _ _ _
We hope that this Blog has been both relevant and helpful to you.
The MTSS process is a critical process that is pivotal to the learning and progress of many struggling students across this country.
We continually work with a wide variety of districts and schools to help them evaluate the current status and efficacy of their MTSS systems and outcomes, and to strategically and systematically guide them to “the next level of MTSS excellence.”
The MTSS improvement process never ends. . . especially as students’ challenges increase in scale and complexity, and new interventions and approaches are released every month.
If you and your team would like to discuss your goals and needs in preparation for the new year, I am happy to provide a free hour of consultation. . . now or into the Summer.
If you are interested in our MTSS Implementation Guidebook or our on-line/on-demand MTSS Design and Implementation course (with a free 35-minute Introductory Webinar), feel free to CLICK on the LINKS below:
Publications to Help You Succeed - Project ACHIEVE
Free Webinar: Effective MTSS Systems of Support - Project ACHIEVE
Meanwhile, thanks for reading my Blog.
Best,